Station Title: Unilateral Upper Limb Neuropathy
Duration: 10 Minutes (2 minutes reading, 8 minutes performance)
Learning Objectives: * Perform a structured hand and neurological examination.
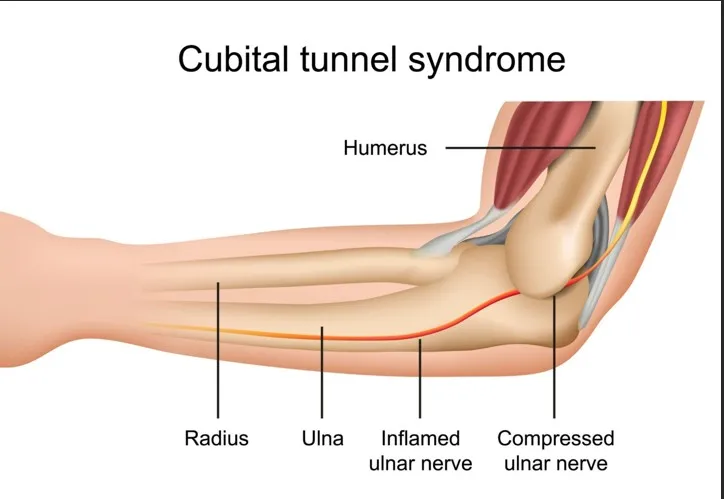
- Differentiate between Carpal Tunnel Syndrome (Median Nerve) and Cubital Tunnel Syndrome (Ulnar Nerve).
- Demonstrate professional communication and clinical reasoning via “running commentary.”
Patient Profile
- Name: Mr. David Miller
- Age: 42 years old
- Occupation: Factory Assembly Line Worker (repetitive manual tasks)
- Ethnicity: Caucasian
- Social History: Smokes 10 cigarettes/day; drinks 3–4 beers on weekends.
Presenting Complaint
“My right hand has been feeling tingly and numb for the last three months. It’s getting harder to do my job because my grip feels weak.”
Contextual Information
- History of Presenting Complaint (HPC): Symptoms are worse at night and after a long shift. Numbness mainly affects the ring and pinky fingers. He denies any neck pain or radiation from the shoulder.
- Past Medical History (PMH): Type 2 Diabetes (HbA1c 7.4%), Hypertension.
- Medications: Metformin 500mg BD, Amlodipine 5mg OD.
- Allergies: Nil.
Exam Instructions
Candidate Instructions
David Miller presents with a 3-month history of right-hand numbness. A brief history has already been taken.
- Perform a focused physical examination of the right upper limb to determine the cause of his symptoms.
- Provide a running commentary to the examiner.
- State your provisional diagnosis and two differential diagnoses to the patient.
- Briefly outline the next steps in management.
Standardised Patient (SP) Instructions
- Demeanour: Concerned but cooperative.
- Physical Findings: When the candidate tests sensation, do not say “I can’t feel it.” Simply remain silent when they touch the tip of your little finger and the ulnar border of the hand.
- Motor: Act “clumsy” when asked to spread your fingers. When performing the “Paper Test” (Froment’s), you cannot keep your thumb flat; you must bend the tip of your thumb to hold the paper.
- Pain: Tapping the “funny bone” area (medial elbow) causes a mild “electric shock” sensation down to the pinky.
Examiner Checklist Items
- Washes hands and gains informed consent.
- Inspection: Checks for hypothenar vs. thenar wasting.
- Palpation: Palpates the medial epicondylar groove and the carpal tunnel.
- Motor: Tests finger abduction (First Dorsal Interosseous) and thumb abduction (APB).
- Sensory: Checks sensation at the tip of the index (Median) and pinky (Ulnar).
- Special Tests: Performs Froment’s Sign, Elbow Flexion Test, and Tinel’s at the elbow.
- Reasoning: Correctly identifies Ulnar nerve entrapment at the elbow.
Key Clinical Findings
- Vitals: Stable.
- Inspection: Mild wasting of the hypothenar eminence. No thenar wasting.
- Motor: Weakness in right finger abduction (4/5).
- Sensory: Reduced light touch/pinprick over the 5th digit and ulnar half of the 4th digit.
- Special Tests: * Positive Froment’s Sign (Thumb IP joint flexes).
- Positive Tinel’s Sign at the cubital tunnel.
- Negative Phalen’s and Tinel’s at the wrist.
Communication Triggers (Murtagh Approach)
- Open-Ended Start: “Before I begin the exam, could you show me exactly where the numbness is most bothersome?”
- Signposting: “I am now going to test the strength in your fingers to see if the nerves are sending signals correctly.”
- Empathy: “I understand this is affecting your work; we will get to the bottom of this today.”
- Lay Language: Instead of “Interosseous wasting,” say “some thinning of the muscles in the fleshy part of your hand.”
Assessment & Marking Guide
| Criteria | Satisfactory | Superior |
| Structure | Follows Look, Feel, Move. | Seamless flow with running commentary. |
| Neurological | Checks Median and Ulnar nerves. | Differentiates between wrist and elbow sites. |
| Special Tests | Performs at least one nerve-specific test. | Performs Tinel’s, Elbow Flexion, and Froment’s. |
| Diagnosis | Identifies nerve issue. | Diagnoses Cubital Tunnel Syndrome. |
| Differentials | Mentions “nerve entrapment.” | Lists DM Neuropathy and Cervical Radiculopathy. |
Sample Answers / Model Performance
Clinical Reasoning Commentary
“On inspection, I note mild hypothenar wasting but the thenar eminence is spared, which points away from Carpal Tunnel. Sensation is decreased in the ulnar distribution. Positive Froment’s sign suggests Ulnar nerve palsy. Since Tinel’s is positive at the elbow and negative at the wrist, the entrapment is likely at the Cubital Tunnel.”
Explanation to Patient
“David, based on the exam, I believe your ulnar nerve—often called the ‘funny bone’ nerve—is being squeezed at your elbow. This is called Cubital Tunnel Syndrome. It is likely related to the repetitive movements at your job. Because you have diabetes, the nerves can also be a bit more sensitive. I’d like to organize a ‘nerve conduction study’ (an electrical test of the wires in your arm) to confirm this and then discuss some elbow bracing or workplace adjustments.”